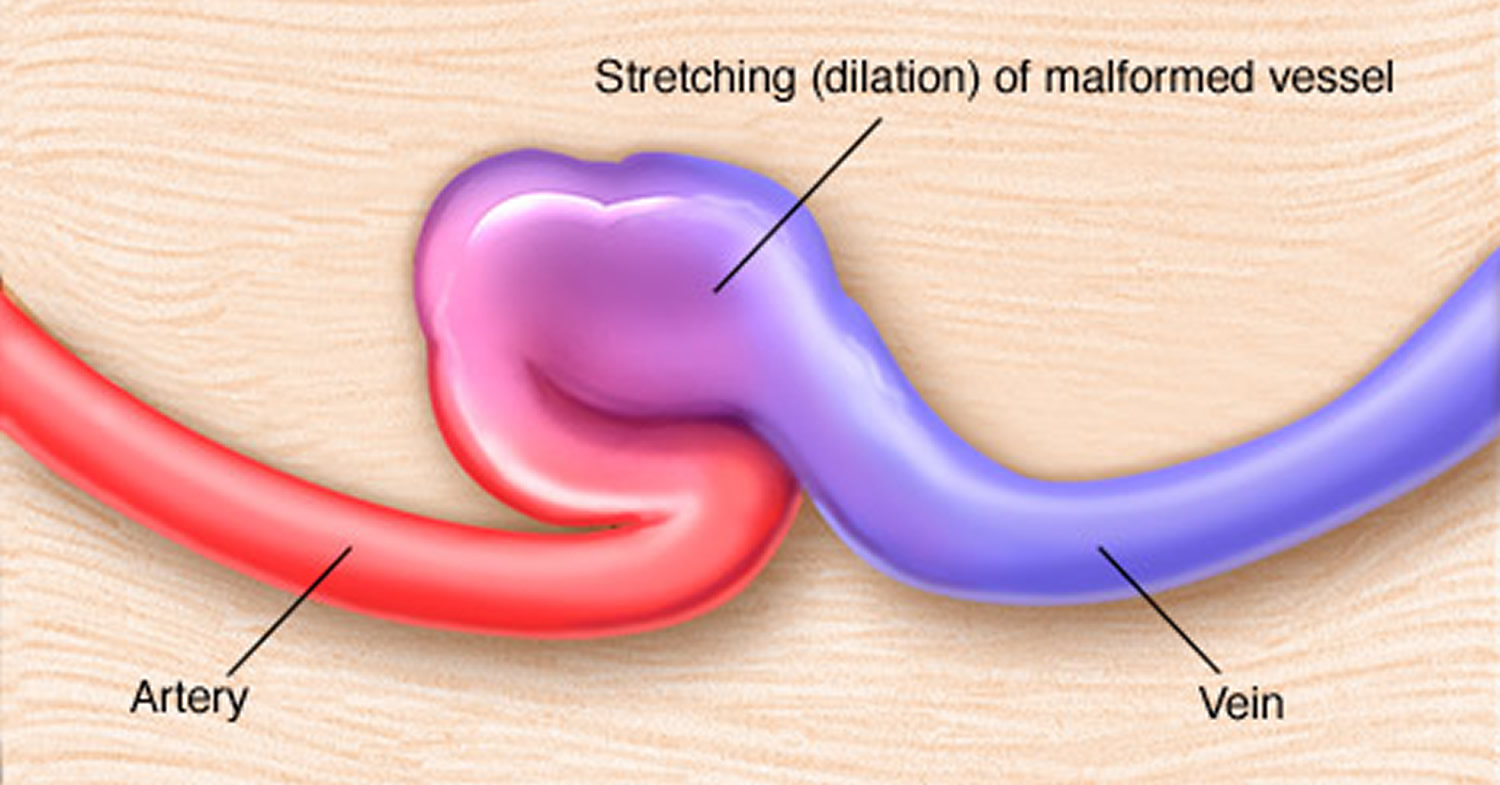
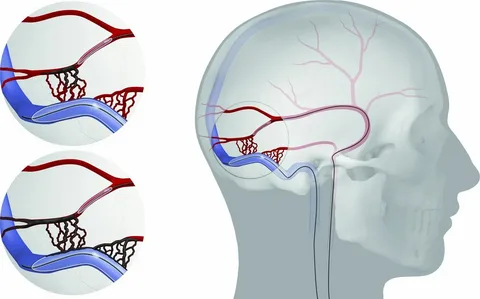
A dural arteriovenous fistula (dAVF) is an abnormal direct connection between arteries and veins within the dura mater—the tough membrane covering the brain and spinal cord. Unlike AVMs, which are congenital, dAVFs are typically acquired conditions that develop in response to venous sinus thrombosis, trauma, surgery, or infection.
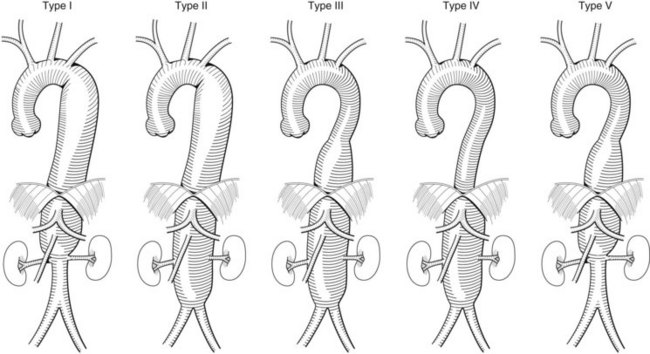
dAVFs are classified using the Cognard or Borden grading systems based on their venous drainage pattern, which determines their clinical risk. Fistulas draining into venous sinuses with normal flow direction (Cognard Type I) carry minimal risk, while those with cortical venous reflux (Cognard Types IIb–V) carry a significant risk of hemorrhage, venous infarction, and progressive neurological deterioration.
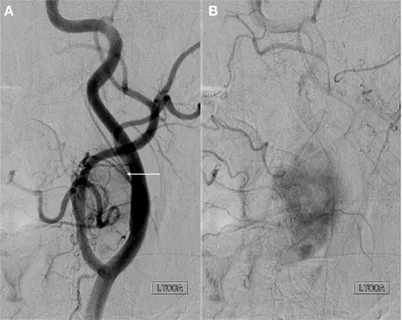
Some complex dAVFs benefit from a combined approach—embolization to reduce flow through the fistula followed by microsurgical disconnection—performed in a hybrid operating room that combines the capabilities of an angiography suite with a neurosurgical operating theater.
Many patients with pulsatile tinnitus caused by dAVFs have been told their symptoms are “just tinnitus” or have been given hearing aids without an adequate vascular workup. If you have pulsatile tinnitus that beats in time with your heartbeat, a thorough evaluation including advanced imaging can identify treatable causes. Dr. Choudhri established a dedicated multidisciplinary Pulsatile Tinnitus Program and has published diagnostic imaging algorithms for this condition.