
Pulsatile tinnitus is a rhythmic sound in one or both ears that beats in time with your heartbeat. Patients describe it as whooshing, thumping, pulsing, or a rushing water sound. Unlike ordinary tinnitus—which is typically a constant ringing or buzzing caused by damage to the inner ear—pulsatile tinnitus almost always has an identifiable, vascular cause.
This means pulsatile tinnitus is not something you simply have to live with. In the majority of cases, the underlying cause can be found through proper investigation, and in many cases, it can be treated or cured entirely.
If you have been told that pulsatile tinnitus is “just tinnitus,” that there is nothing that can be done, or that you should simply learn to cope—you may not have received a complete evaluation. A thorough neurovascular workup can identify treatable causes that are missed by standard ENT or audiology assessments.
Pulsatile tinnitus can be caused by a variety of vascular conditions, some of which carry real health risks. A specialist evaluation is important to determine which cause is present and whether treatment is needed.
An abnormal connection between arteries and veins in the covering of the brain, often located near the ear at the transverse-sigmoid sinus junction. dAVFs are one of the most important causes of pulsatile tinnitus to identify because some types carry a risk of stroke or brain hemorrhage. The good news: dAVFs are highly curable through minimally invasive endovascular embolization, with many patients experiencing immediate resolution of their pulsatile tinnitus after treatment.
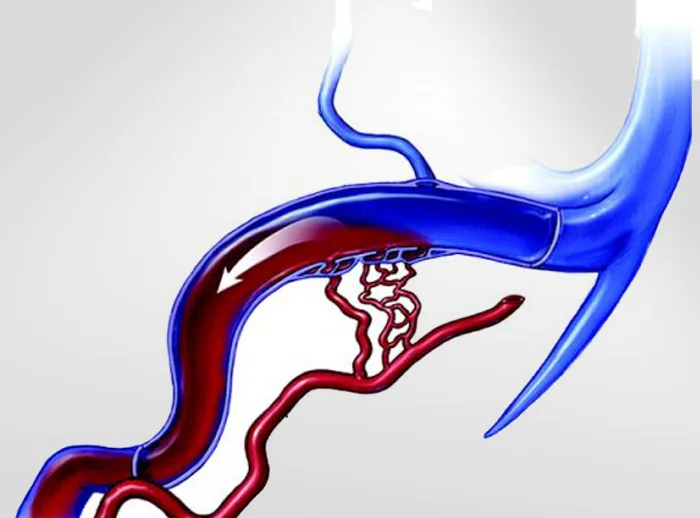
Narrowing of the large veins that drain blood from the brain can create turbulent blood flow near the ear. This turbulence is what you hear as a pulsing sound. Venous stenosis is frequently associated with idiopathic intracranial hypertension (IIH) and can cause headaches, visual disturbances, and pulsatile tinnitus. Treatment with venous sinus stenting can relieve symptoms.
A small outpouching or pocket in the wall of a venous sinus, typically near the sigmoid sinus close to the ear. Blood swirling through this outpouching creates turbulent flow that you hear as pulsatile tinnitus. While not dangerous, diverticula can cause severely debilitating symptoms. Endovascular treatment with coil embolization of the outpouching can resolve the tinnitus while preserving normal sinus flow.
Elevated pressure around the brain without a structural cause. Patients experience severe headaches, pulsatile tinnitus, visual disturbances, and risk of permanent vision loss. IIH is increasingly understood to involve venous sinus stenosis, and treatment options include medications (acetazolamide), emerging therapies (GLP-1 receptor agonists like semaglutide), venous sinus stenting, and shunting.
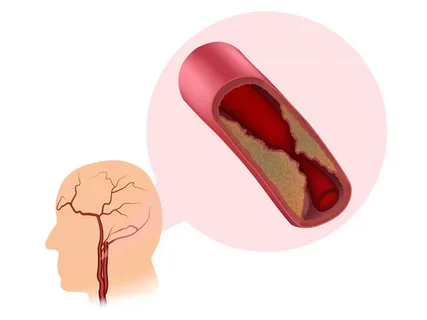
Plaque buildup in the carotid arteries can create turbulent blood flow that you hear as pulsatile tinnitus. Identified through carotid ultrasound and treated with surgical or endovascular revascularization if significant.
A rare, typically benign tumor rich in blood vessels that grows near the ear (glomus tympanicum or glomus jugulare). Treatment may involve surgery, embolization, radiosurgery, or observation depending on size and location.
Our published diagnostic algorithm for pulsatile tinnitus guides the sequence and selection of imaging based on clinical findings.
For patients whose initial imaging suggests a vascular cause—or when initial imaging is normal but clinical suspicion remains high—catheter-based cerebral angiography provides the highest-resolution view of the brain’s blood vessels. This minimally invasive procedure is typically performed through a small puncture in the wrist and can identify dural fistulas, venous stenosis, and other causes that are invisible on non-invasive imaging.
Dr. Choudhri has pioneered the use of balloon-assisted retrograde cerebral phlebography—an advanced catheter-based technique for visualizing the cerebral venous system with unprecedented detail. This technique can reveal venous diverticula, subtle stenoses, and emissary vein anatomy that conventional angiography may miss. It has been presented at the SNIS Cerebral Venous and CSF Disorders Summit and the North American Skull Base Society meeting.
Many patients with pulsatile tinnitus have been told their imaging is “normal”—but standard imaging may not include the specialized venous protocols needed to identify the cause. If you have had an MRI or CT that was read as normal but your symptoms persist, a more targeted evaluation may reveal the answer.

Treatment depends entirely on the underlying cause. The encouraging news is that many causes of pulsatile tinnitus are highly treatable, and in some cases, curable.
Most endovascular procedures are performed through the wrist (transradial or transulnar access), allowing patients to sit up and walk immediately after the procedure.
