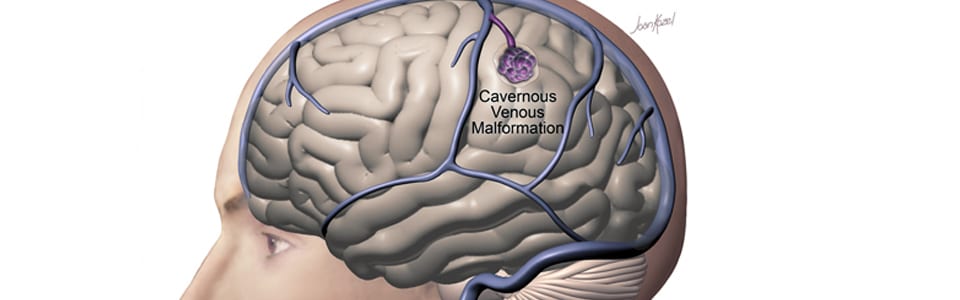
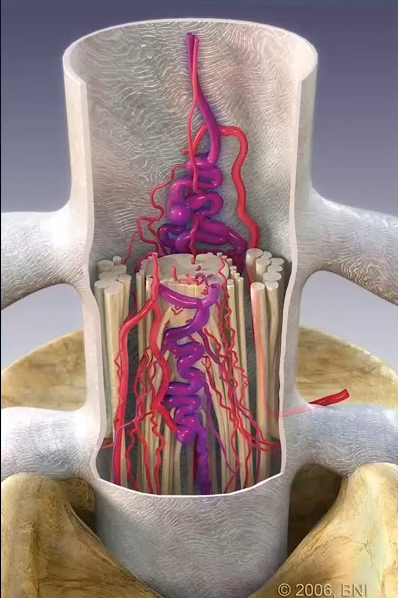
A cavernous malformation (also called a cavernoma or cavernous angioma) is a cluster of abnormally formed, thin-walled blood vessels in the brain or spinal cord. Unlike AVMs, cavernous malformations are low-flow lesions—they do not have the high-pressure arterial blood flow that makes AVMs dangerous. However, they can bleed (usually small hemorrhages), causing headaches, seizures, and neurological deficits depending on their location.
Cavernous malformations are found in approximately 0.5% of the general population. They can occur anywhere in the brain, but those located in the brainstem or deep brain structures pose the greatest challenge due to the critical functions of surrounding tissue.
Symptoms
Seizures — the most common symptom, especially for superficial cortical lesions
Headaches — may follow episodes of minor bleeding
Progressive neurological deficits — weakness, numbness, vision changes, or balance problems, particularly with brainstem cavernomas
Hemorrhage — typically small, repeated bleeds that cause cumulative damage
Incidental discovery — many are found on MRI performed for other reasons
Diagnosis
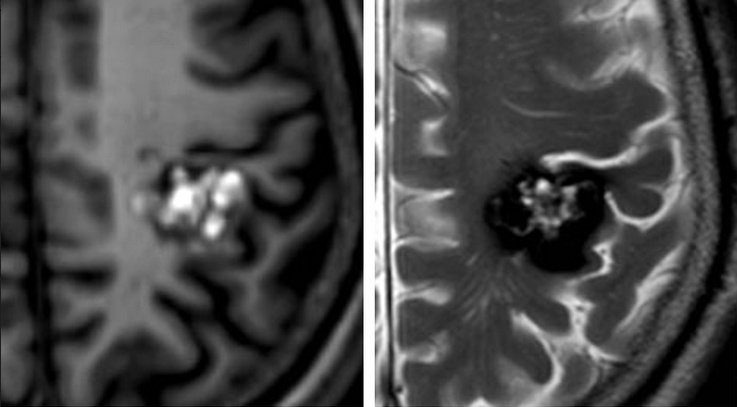
MRI with Susceptibility-Weighted Imaging (SWI): The diagnostic standard for cavernous malformations. The characteristic “popcorn” appearance with a dark hemosiderin ring on MRI is essentially diagnostic.
Genetic Testing: Recommended for patients with multiple cavernous malformations, as familial forms (CCM1, CCM2, CCM3 gene mutations) account for up to 20% of cases.
Notably, cavernous malformations are typically invisible on catheter angiography, which distinguishes them from AVMs and dural fistulas.
Treatment Options
Microsurgical Resection
Surgery is the primary treatment for symptomatic cavernous malformations and provides a definitive cure when complete resection is achieved. The decision to operate balances the risks of the lesion’s natural history (ongoing seizures, progressive hemorrhage) against the risks of surgery, which depend heavily on location. Dr. Choudhri has specific expertise in the resection of challenging brainstem cavernous malformations, utilizing CO2 laser technology, neuronavigation, and continuous neurophysiological monitoring to remove these lesions while preserving the delicate brainstem pathways. He published early work on the flexible omnidirectional CO2 laser for resection of brainstem, supratentorial, and intramedullary cavernous malformations during his training at Stanford.
Brainstem cavernous malformations are among the most technically demanding lesions in neurosurgery. Dr. Choudhri has published peer-reviewed studies on techniques including endoscopic-assisted approaches and gravity-retraction positioning strategies to safely access these deep-seated lesions.
Stereotactic Radiosurgery
For deep-seated cavernous malformations where surgery carries unacceptable risk, radiosurgery may reduce the rate of future hemorrhage. However, the evidence base is less robust than for AVMs, and radiosurgery does not eliminate the lesion. It is generally reserved for patients with repeated hemorrhages from surgically inaccessible locations.
Observation
Many cavernous malformations—especially incidental, asymptomatic, superficial lesions—can be safely monitored with periodic MRI. The decision framework considers hemorrhage history, seizure burden, lesion location, and patient preference.